Frequently Asked Questions
- Thyroid Nodule
- Hypoglycemia
- Adrenal Adenoma (Mass)
- Hashimoto's Disease
- Cushing's Disease
- Pituitary Tumors (Adenoma)
- Osteoporosis
- Hypothyroidism
- Hyperthyroidism
- Managing your Cholesterol
- Diabetes
- Fine Needle Aspiration (FNA)
Thyroid Nodule
Risk factor for thyroid cancer are:
- People over 65 year old
- Men
- Children
- History of XRT exposure to the neck
- History of thyroid cancer in a first degree family member
Findings on sonogram suspicious are:
- Hypoechoic
- Microcalcification
- Vascular flow
- Irregular borders
- Taller than wide
Fine needle aspirations are recommended by the American Thyroid Association based on patients risks category.
Hypoglycemia
- Fasting hypoglycemia
- Reactive hypoglycemia
Of the two, the most common one is reactive hypoglycemia, usually occurs 2-4 hours after a meal usually high in carbohydrates, patient feels jittery and diaphoretic, this is confirmed with a low glucose reading, and relief with the intake of carbohydrates.
Patients that have glucose intolerance, knows as pre-diabetics are prone to develop this kind of hypoglycemia. Most of the times changing the eating habits and having a more balanced diet, high in protein and low in carbohydrates can avoid the hypoglycemia. In case we can’t avoid with the diet, precose is an alternative with good results for this group of patients. In case it is not related to food a 12-14 hours fasting blood test is ordered or when the patient has the symptoms to rule out unusual conditions such as insulinoma.
Now a days procedures such as gastric bypass have becoming so popular we are seen hypoglycemia as a complication of this procedure, many cases have been reported in the New England Journal of Medicine, some of them become so difficult to treat, that one of the alternative for some of these patients have been partial removal of the pancreas.
Adrenal Adenoma (Mass)
The prevalence of adrenal incidentaloma is higher in older patients (10%).
In a large study done with a total of 1800 pts with adrenal masses, reviewed published articles from 820 journal from 1980- 2008, of all the masses, these were the percentages:
Benign:
- Non Functional: 89.7%
- Subclinical Cushing: 6.4%
- Pheochromocytoma: 3.1%
- Primary aldosteronism: 0.6%
Malignant:
- Primary Adrenal Cancer: 1.9 %
- Metastasis: 0.7%
- Approximately 15% to 20% of aldosterone-secreting adenomas (>1.5 cm) consecrate cortisol
Hashimoto's Disease
Some clinicians reserve this term for patients with goiter and hypothyroidism. However, many patients do not have hypothyroidism, and others have no goiter or even have an atrophic thyroid gland. These are considered manifestations of the same disease with differing clinical phenotypes. Hashimoto’s thyroiditis is primarily a disease of women, with a sex ratio of approximately 7:1; it can also occur in children.
The usual course of Hashimoto’s thyroiditis is gradual loss of thyroid function. Among patients with this disorder who have mild (subclinical) hypothyroidism, exhibited as slight increases in TSH and the presence of thyroid antibodies, overt hypothyroidism occurs at a rate of about 5 percent per year .
Variant mild forms of Hashimoto’s thyroiditis include silent (or painless) thyroiditis and postpartum thyroiditis, both of which are transient but may be followed years later by thyroid failure.
Cushing's Disease
Usually ACTH-secreting tumors are benign and are microadenomas under 10 mm; 50% of them are 5 mm or less.These tumors are almost always benign and are usually microadenomas (ie, <10 mm in diameter); in 30 to 40%, the microadenoma is so small that it is not detectable by magnetic resonance imaging (MRI), while in 10 to 15% a macroadenoma is present.
Treatment is aimed first at the anterior pituitary gland. For most adult patients with Cushing’s disease, we suggest transsphenoidal surgery with an experienced surgeon as primary therapy. MRI is performed preoperatively to try to locate the pituitary tumor. However, surgery should be performed even if a tumor is not visualized.
The extent of surgery varies. Ideally, the entire tumor is removed while normal pituitary tissue is left behind. However, in adult patients in whom a microadenoma cannot be identified at the time of surgery and for whom fertility is not an issue, 80 to 90% of the pituitary should be resected, leaving a small island attached to the stalk.
Since most plasma ACTH assays cannot reliably detect subnormal or suppressed levels, experts suggest proceeding with adrenal imaging in patients with endogenous hypercortisolism who have ACTH concentrations less than 25 pg/mL.
A consensus statement by Cushing’s syndrome experts suggested that inferior petrosal sinus sampling be performed in any patient with a pituitary lesion smaller than 6 mm. With an experienced neurosurgeon,surgery for Cushing’s patients can achieve an initial cure rate of 80 to 90% with microadenomas, but less than 60% with macroadenomas. A frankly elevated midnight cortisol concentration—either in serum or saliva—is highly indicative of true Cushing’s syndrome.
Pituitary Tumors (Adenoma)
PITUITARY ADENOMAS:
- Prolactinomas: 60%
- Growth Hormone: 20%
- Acth (Cushing’s Disease): 10%
- Nonfunctional 10%: (Some of them may in fact be gonadotropin – secreting or alpha subunits -secreting adenomas)
Hypersecretion of TSH, gonadotropin or alpha subunits – secreting adenomas are unusual. Initial evaluation consist in hormonal evaluation and based on results the plan of action. Some of them are just treated with medical treatment and have better results than surgery like the prolactinomas, and some of them require surgery.
Depending of some studies 10% to 30% of pituitary adenomas are clinically nonfunctioning or “silent,” and of these, 80% to 90% are of gonadotroph cell origin. Most of the ACTH-secreting pituitary tumors are usually benign microadenomas < 10 mm; 50% are ~ 5 mm or less. Thyrotropin -secreting pituitary adenomas are very rare; they are often very large tumors (macroadenomas).
Most gonadotroph tumors predominantly secrete FSH and the alpha subunit and are macroadenomas. Most gonadotroph tumors present with effects of the tumor mass itself. Tumor mass effects include vision abnormalities due to compression of the optic chiasm, headache, or signs and symptoms of hypopituitarism caused by pituitary gland compression. Gonadotroph tumors are usually large at presentation and up to 60% of patients have biochemical evidence of hypopituitarism at diagnosis.
Osteoporosis
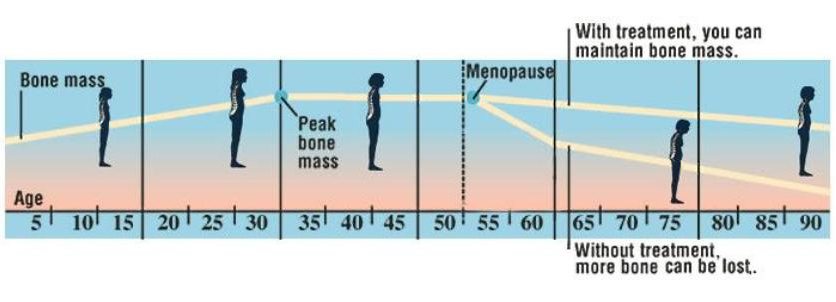
Childhood
The body builds the most bone during these years. That’s why boys and girls need foods rich in calcium. They also need plenty of exercise. A healthy diet and exercise helps bones grow strong.
Young Adulthood to Age 30
During young adulthood, bones become their strongest. This is called peak bone mass. The same habits that kept bones healthy in childhood help keep bone healthy in adulthood.
Age 30 to Menopause
Bone mass declines slightly during these years. Your body makes just enough new bone to maintain peak bone mass. To keep your bones at their peak mass, be sure to exercise and get plenty of calcium.
After Menopause
Menopause is when a woman stops having monthly periods. After menopause, the body makes less estrogen (female hormone). This increases bone loss. At this point, treatment may be needed to reduce risk of fracture. Exercise and calcium can also help keep your bones strong.
Later in Life
In later years, both men and women need to take extra care of their bones. By this point, the body loses more bone than it makes. If too much bone is lost, you may be at risk for fractures. You can lessen bone loss by staying active and increasing your calcium intake. If you have osteoporosis, you can also learn ways to increase everyday safety.
Hypothyroidism
Signs of hypothyroidism (too little thyroid hormone):
- Fatigue or sluggishness
- Difficulty concentrating or thinking clearly; forgetfulness
- Dry skin, hair loss
- Depression
- Unexpected weight gain
- Feeling overheated
HOME CARE:
- Take your medicine exactly as directed at the same time every day. Don’t take thyroid pills with soy milk since this interferes with absorption.
- After taking your thyroid medicine:
- Wait 1-2 hours before eating or drinking anything that contains soy.
- Wait 4 hours before taking iron supplements, antacids that contain either calcium or aluminum hydroxide, or calcium supplements (regular amounts of cow’s milk are probably okay).
- Do not stop treatment on your own. If you do, your symptoms will return.
- Eat a high-fiber, low-calorie diet to relieve constipation and maintain a healthy weight.
- Get regular exercise. Talk to your doctor about an exercise program that is right for you.
FOLLOW UP with your doctor or as advised by our staff. Your thyroid level will need to be monitored for the rest of your life. During your routine visits, tell your doctor about any symptoms such as the ones listed below.
GET PROMPT MEDICAL ATTENTION if any of the following occur:
- Extreme fatigue
- Puffy hands, face, or feet
- Chest pain or trouble breathing
- Palpitations or irregular heartbeat
- Confusion or loss of consciousness
Hyperthyroidism
Signs of hyperthyroidism (too much thyroid hormone, which can be a side effect of treatment for low thyroid):
- Restlessness, nervousness, tremor
- Increased appetite with weight loss
- Excess sweating
- Palpitations or irregular heartbeat
- Feeling cold, or cold hands and/or feet
HOME CARE:
- Take your medicine exactly as directed at the same time every day.
- Keep your pills in a container that is labeled with the days of the week. This will help you remember whether you’ve taken your medicine each day.
- Never stop treatment on your own. If you do, your symptoms will return.
FOLLOW UP with your doctor or as advised by our staff. Your thyroid level will need to be monitored for the rest of your life. During your routine visits, tell your doctor about any symptoms such as the ones listed below.
GET PROMPT MEDICAL ATTENTION if any of the following occur:
- Loss of consciousness
- Extreme fatigue
- Puffy hands, face, or feet
- Chest pain or shortness of breath
- Trouble breathing
- Fast or irregular heartbeat
- Confusion
Managing your Cholesterol
Checking Your Cholesterol
Your cholesterol is checked with a simple blood test. The results tell you how much cholesterol you have in your blood. Get checked as often as your healthcare provider suggests. As you work to lower your cholesterol, your numbers will change slowly. But they will change. Be patient and stay on track.
Your Total Cholesterol Number
A blood test will give you a number for the total amount of cholesterol in your blood. The higher this number, the more likely it is that cholesterol will build up in your blood vessels. For your health, it is suggested that your total cholesterol be lower than 200 . Even if your cholesterol is just slightly high, you are at increased risk for health problems.
My total cholesterol is: ________________
Your Lipid Numbers
Total cholesterol is just one part of the story. Cholesterol is made up of different kinds of fats, or “lipids.” If your total cholesterol is high, knowing your lipid profile is important. The two most important lipids are HDL and LDL. Lipids are checked during a “fasting” blood test (you don’t eat for a certain amount of time before the test is done). And along with cholesterol, triglyceride (another type of fat) can also lead to blocked arteries. So, knowing your HDL, LDL, and triglyceride numbers as well as your total cholesterol gives you a more complete picture of your cholesterol level.
- HDL is called the “good” cholesterol. It moves out of the bloodstream and does not block your blood vessels. HDL levels are affected by how much you exercise and what you eat. For most people, HDL should be 40 or higher if you’re a man and 50 or higher if you’re a woman.
- My HDL cholesterol is: ________________
- LDL is called the “bad” cholesterol. This is because it can stick to your artery walls and block blood flow. LDL levels are most affected by what you eat. For most people, LDL should be lower than 100.
- My LDL cholesterol is: ________________
- Triglyceride is a type of fat the body uses to store energy. Too much triglyceride can increase your risk for heart disease. Triglyceride levels should be under 150.
- My triglyceride is: ________________
Diabetes
GENERAL INFORMATION ABOUT DIABETES:
Cells of the body need glucose (sugar) for fuel. Insulin is the hormone in the body that lets glucose move from the blood into the cells. Diabetes is a chronic health condition where the body is not able to produce enough insulin, or does not respond well to its own insulin. Because the glucose in the blood cannot get into the cells, it builds up in the blood causing high blood sugar (hyperglycemia).
If there is not enough insulin, or if the body stops responding to insulin, sugar builds up in the blood. That is what happens to people with diabetes.
There are 2 different types of diabetes. In type 1 diabetes, the problem is that the body makes little or no insulin. In type 2 diabetes, the problem is that:
- The body’s cells do not respond to insulin
- The body does not make enough insulin
- Or both
Your actual blood sugar level is a result of the balance between several factors. These include what kind of food you eat and how much of it you eat, how much exercise you get, and the amount of insulin present in your body. Eating too much of the wrong kinds of food or not taking diabetes medicine on time can cause high blood sugar. Infections can cause high blood sugar even if you are taking medicines correctly. Missing meals, not eating enough food, or taking too much diabetes medicine can lead to low blood sugar.
Untreated over long periods of time, diabetes can cause serious problems such as heart disease, stroke, kidney failure, blindness, nerve pain or loss of feeling in the legs and feet, and gangrene of the feet. With good treatment keeping your blood sugar under control, you can prevent or delay the complications of diabetes. Normal blood sugar levels are between 90-130 before a meal and not more than 180 two hours after a meal.
HOME CARE:
1) Follow your prescribed diabetic diet and take insulin or oral diabetic medicine exactly as ordered.
2) Monitor blood sugars as advised. Keep a log of your results. This will help your doctor adjust your medicines to keep your blood sugar under control.
3) Try to achieve your ideal weight. Proper diet and exercise can reduce or eliminate the need to take diabetes medicine.
4) Avoid tobacco smoking, which worsens the effect of diabetes on your circulation. The risk of a heart attack in a diabetic is 15 times more likely if you smoke.
5) Pay attention to good foot care. If you have lost feeling in your feet you may not notice an injury or infection. Check your feet and between your toes at least once a week.
6) Wear a Medic-Alert bracelet or carry a card in your wallet explaining that you are diabetic. In the event that you become very ill and are unable to give this information, it will help medical personnel provide proper care.
7) If you become ill with an infection (viral or bacterial), check your blood sugar often. If the blood sugar is above your usual range, and if you take insulin, use the “sliding scale” dose of regular (R) insulin dose your doctor gave you. Recheck your blood sugar in four hours. If you do not take insulin or if no “sliding scale” instructions were given, contact your doctor for further advice.
8) Always carry a source of high sugar food with you in case you get symptoms of low blood sugar again. At the first sign of low blood sugar, eat the sugar source to raise your blood sugar while you seek medical help. Examples of high sugar foods include:
Glucose tablets (found at most drug stores), non-diet cola drinks (Coke, Pepsi, Root Beer, etc.), milk chocolate candies, hard candies, orange juice or apple juice with added sugar.
Check your blood sugar 20 minutes after treating yourself. If it is still low, go to an emergency room.
9) If you are not able to eat due to illness, loss of appetite or vomiting, you MUST reduce your diabetes medicine. If you take oral diabetes medicine, stop your pills and contact your doctor. If you take insulin, contact your doctor to ask for a temporary adjustment of your dose. If there is a delay in reaching your doctor, reduce your daily insulin dose to ONE-HALF (½) of what you usually take. Monitor your blood sugar every 4-6 hours, until you are able to begin eating again normally.
FOLLOW UP with your doctor as advised . For more information, contact the American Diabetes Association. www.diabetes.org or (800-DIABETES). You can get a Medic-Alert bracelet from www.medicalert.org (800) 432-5378.
GET PROMPT MEDICAL ATTENTION if any of the following occur:
— HIGH BLOOD SUGAR: frequent urination, dizziness, drowsiness, thirst, headache, nausea or vomiting, abdominal pain, vision changes, fast breathing, confusion or loss of consciousness
— LOW BLOOD SUGAR: fatigue, headache, shakes, excess sweating, hunger, feeling anxious or restless, vision changes, drowsiness, weakness, confusion or loss of consciousness
— Chest pain or shortness of breath
— Dizziness or fainting
— Weakness of an arm or leg or one side of the face
— Trouble with speech or vision
GENERAL INFORMATION ABOUT DIET FOR DIABETICS:
Food is an important tool that you can use to control diabetes and stay healthy. Eating well-balanced meals in the correct amounts will help you control your blood glucose levels and prevent low blood sugar reactions. It will also help you reduce the health risks of diabetes. A registered dietitian (RD) will explain the diabetes diet and help you plan meals and snacks that are healthy to eat. If you have any questions, do not hesitate to call the dietitian for advice.
GUIDELINES FOR SUCCESS:
 Consult with your doctor before you starting a diabetes diet or weight loss program. If you have not yet consulted a dietitian, ask your doctor for a referral.
Consult with your doctor before you starting a diabetes diet or weight loss program. If you have not yet consulted a dietitian, ask your doctor for a referral.- Select foods from the six food groups. Your dietitian will advise you on food choices within each group, serving sizes and how many servings you can have at each meal.
- Grains, beans and starchy vegetables
- Vegetables
- Fruit
- Milk or Yogurt
- Meats
- Fats, sweets and alcohol (only a small amount from this group)
- Monitor your blood sugar levels as requested by your doctor. Take any medicine as prescribed by your doctor.
- Learn to read nutrition labels and select appropriate portion sizes.
- Eat only the amount of food in your meal plan. Eat about the same amount of food at regular times each day. Do not skip meals. Eat meals 4 to 5 hours apart, with snacks in between.
- Limit alcohol. It raises blood sugar levels. Drink water or calorie-free diet drinks that use safe sweeteners.
- Eat less fat to help lower your risk of heart disease. Use nonfat or low-fat dairy products and lean meats. Avoid fried foods. Use cooking oils that are unsaturated.
- Talk to your nutritionist about safe sugar substitutes.
- Avoid added salt. It can contribute to high blood pressure, which can cause heart disease. People with diabetes already have a risk of high blood pressure and heart disease.
- Maintain a healthy weight. If you need to lose weight, cut down on your portion sizes. But do not skip meals. Exercise is an important part of any weight management program. Talk to your doctor about an exercise program that is right for you.
- For more information about the best diet plan for you, talk with a registered dietitian (RD). To obtain a referral to an RD in your area, contact your insurance.
What Is the A1C Test?
Using your meter helps you track your blood sugar every day. But you also need to know if your treatment plan is keeping you healthy over time. An A1C (glycated hemoglobin) test can help. This test measures your average blood sugar level over a few months. A higher A1C result means that you have a higher risk of developing complications.
The A1C test
The A1C is a blood test done by your healthcare provider. You will likely have an A1C test every 2 to 3 months.
Your Blood Glucose Goal
A1C has been shown as a percentage. But it can also be shown as a number representing the estimated Average Glucose (eAG). Unlike the A1C percentage, eAG is a number similar to the numbers listed on your daily glucose monitor. Both A1C and eAG measure the amount of glucose stuck to a protein called hemoglobin in red blood cells. Your healthcare provider will help you figure out what your ideal A1C or eAG should be. Your target number will depend on your age, general health, and other factors. If your current number is too high, your treatment plan may need changes, such as different medications.
Sample Results
Most people aim for an A1c lower than 7%. That’s an eAG less than 154 mg/dL.
Fine Needle Aspiration (FNA)
FINE NEEDLE ASPIRATION OF THE THYROID
Fine needle aspiration of the thyroid gland is a procedure to remove thyroid cells for examination. The thyroid gland is a butterfly-shaped gland located inside the front of the lower neck.
This test is usually an outpatient procedure. Numbing medicine (anesthesia) may or may not be used. Because the needle is very thin, you may not need this medicine.
You will lie on your back with a pillow under your shoulders with your neck extended. The biopsy site is sterilized. A thin needle is inserted into your thyroid, where it collects a sample of thyroid cells and fluid. The complete procedure takes approximately 10 minutes. Immediately upon the completion of the procedure you may resume all activities without any restrictions. You will not be required to be fasting.
HOW THE TEST WILL FEEL
If numbing medicine is used, you may feel a sting as the needle is inserted and the medicine is injected. As the biopsy needle passes into your thyroid, you may feel some pressure, but it should not be painful. You may have slight discomfort in your neck afterward. You may also have slight bruising, which soon goes away.
WHY THE TEST IS PERFORMED
This is a test to diagnose thyroid disease or thyroid cancer. It is often used to find out if thyroid nodules that your provider can feel or seen on an ultrasound are noncancerous or cancerous.
Testimonials & Patients
My husband and I were beyond impressed by Dr. Kenneth Shephard and his staff. Everyone from the front desk to the doctor were extremely helpful and kind. We were not rushed at all and we felt as if we were their only patient, which is very rare now a days.
I was very satisfied by Dr. Shephard’s office. The staff and doctor are efficient and welcoming. Dr. Shephard always answered my questions with patience and a smile. He has gone beyond any other doctor I have experienced. He truly cares for his patients.